Nerve regeneration after radical prostatectomy (and the subsequent return of erectile function) usually does take some time, assuming that both nerve bundles around the prostate were able to be preserved by the surgeon. This is because the nerves and arteries that control erections need time to recover and heal. This article explains why this is the case, and what can be done to speed up the healing process.
Introduction to nerve regeneration
Three sets of nerves are important when a man has sex:
- The nerves of penile sensation.
- The nerves that cause an erection.
- The nerves that control climax.
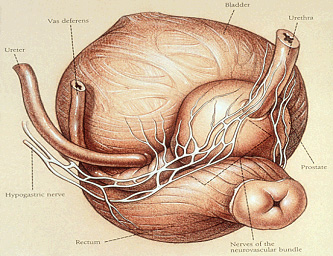
Because of their location, sandwiched between the prostate and the rectum, the second set of nerves can be affected during robotic radical prostatectomy. The other two sets of nerves cannot be affected. Regarding climax after surgery, roughly 80% of men describe climax as being equally satisfying after surgery as before, 10% say that it is better (although no one can explain why!) and 10% say that it is less intense.
Why do nerves need to regenerate if they were not removed?
Nerves can still suffer trauma and minor damage during a radical prostatectomy, even if they were preserved. They need to be delicately separated from the prostate itself which is to be removed, and that does involve bringing them into contact with surgical tools which can leave them stretched, bruised and swollen. This limits how well they work. A good surgeon will of course seek to minimise this, and the more experienced they are of handling nerves, the better the patient outcome. Nerve fibres in this location are also particularly susceptible to damage because they lack the usual myelin sheath (insulation) of most nerves in the body. So some recovery time is required here for the nerves to heal.
The second reason for a recovery period is that the small arteries that travel through the prostate to the erectile mechanism are interrupted when the prostate is removed, so the blood flow through the other arteries to the penis has to increase to allow sufficient blood flow for erections. In some patients this process takes time for the body to adapt to the changes. This is not nerve regeneration specifically, but another aspect of the recovery process that patients should be aware of.
How long does nerve regeneration take?
Recovery of potency may be very rapid in younger patients and is sometimes immediate. However, for most patients the recovery is gradual and can take up to 3 years to plateau, although typically a patient sees a return to erectile function after about 12 months.
Can I do or take anything to speed up nerve regeneration?
I recommend to my patients that they stimulate themselves (or be stimulated by other means) 2-3 times a week and take a Viagra tablet at least once a week as well. This encourages nerve regeneration and increases blood flow to the penis. There are three tablets in the same family as Viagra that you can take: Cialis (tadalafil), Levitra (vardenafil) and Viagra itself (sildenafil). There is evidence that taking one of these tablets regularly after prostate surgery speeds recovery of potency. All three work by increasing blood flow to the penis, and while they won’t give you an erection on their own, they make it easier to get one with stimulation.
Not all patients want to take a tablet for potency and there is no compulsion to do so. Please do be aware that there are common side-effects associated with this increased blood flow, including headaches, facial flushing and indigestion.
About nerve preservation
When is nerve preservation not done?
The term ‘nerve preservation’ or ‘nerve sparing’ during radical prostatectomy refers to preservation of this second set of nerves (the ‘cavernosal nerves’ or ‘neurovascular bundles’ – NVBs). When these nerves are not preserved it is not because they have been accidentally damaged, but because either one (rarely both) or part of one has been removed to ensure that the cancerous cells are fully removed. This is known as ‘cancer control’.
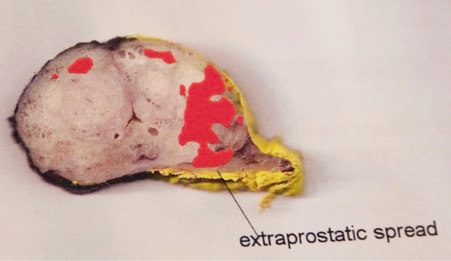
You can see how the location of the prostate cancer on the left side of the prostate specimen below allowed full nerve preservation on this side (you can’t see any tissue on this side because it’s been left behind in the patient) whereas the tumour (depicted as red) on the right side of the prostate was invading the NVB, which meant that NVB removal on this side together with all of the tissue surrounding it was necessary for good cancer control.
Who has nerve preservation?
Patient who are potent (have normal erections) are understandably keen to retain this and so are we. As well as allowing erections following surgery, nerve preservation also allows an earlier return to continence (urinary control) so we always practice nerve preservation whenever the cancer control allows it, which is in about 80% of men. When the cancer is close to one of the nerves we might partially nerve preserve on that side if it is safe to do so and will discuss this with you beforehand if this seems likely.
The decision to nerve preserve is taken after considering the patient’s existing erections, PSA level, biopsy report, MRI scan, rectal examination under anaesthetic immediately before the operation starts and the way the NVB looks and feels during the operation. It is always discussed with patients before surgery.
What are the results of nerve preservation?
I published a study on nerve preservation in 2011 on this – if you’d like to read more, click here to read the article. The results were as follows:
| 40-49 | 50-59 | 60-69 | 70+ | |
|---|---|---|---|---|
| 2 nerves preserved | 100% | 91.8% | 82.9% | 60% |
| 1 nerve preserved | 100% | 66.7% | 50.1% | 0% |
We have also created an interactive results calculator which gives you results charts for cancer cure, potency and continence.
View the Surgery Results Calculator
Other than nerve preservation, what other factors influence potency after surgery?
- Age – the younger the better, as can be seen in the table above.
- The ability to have erections before surgery.
- Medication, especially for elevated blood pressure.
- Other conditions, such as diabetes.
- Psychological factors.
Our clinic specialises in advanced prostate cancer surgery, including nerve-sparing techniques and tailored recovery plans. Contact us to learn more about our prostate cancer procedures.
Looking for more information?
- 9 Common Questions about Prostate Cancer – Get answers to the most pressing questions about prostate cancer, from diagnosis to treatment options.
- What to Expect After a Prostate Cancer Diagnosis – Understand the next steps following your diagnosis, including treatment plans and recovery timelines.
- Prostate Cancer: Diet and Lifestyle Tips for Men – Practical advice on how diet and lifestyle choices can support your recovery and overall health.


